The Ombredanne Inhaler
In many countries specialisation in ansesthesia was not encouraged until comparatively recently. Doubtless one of the reasons for this was the availability of the Ombredanne inhaler, a remarkably foolproof device which, even in relatively untrained hands, gave results which were quite acceptable in its day and age. It has been confused with Clover’s inhaler and its many modifications, but differs so markedly from these in conception and design that it deserves to be better known.
Ombredanne was dissatisfied with the closed inhalers, mainly be- cause the mask frequently had to be raised from the face to admit fresh air. He felt that smooth induction without cyanosis called for a degree of skill not always available and that better results would be obtained if air could be drawn in at each breath, together with grad- ually increasing amounts of ether vapour. Rebreathing was necessary and should increase as the ether concentration rose and it was found better to fill the chamber of the apparatus with sponge soaked in ether so as to get a sufficient concentration.
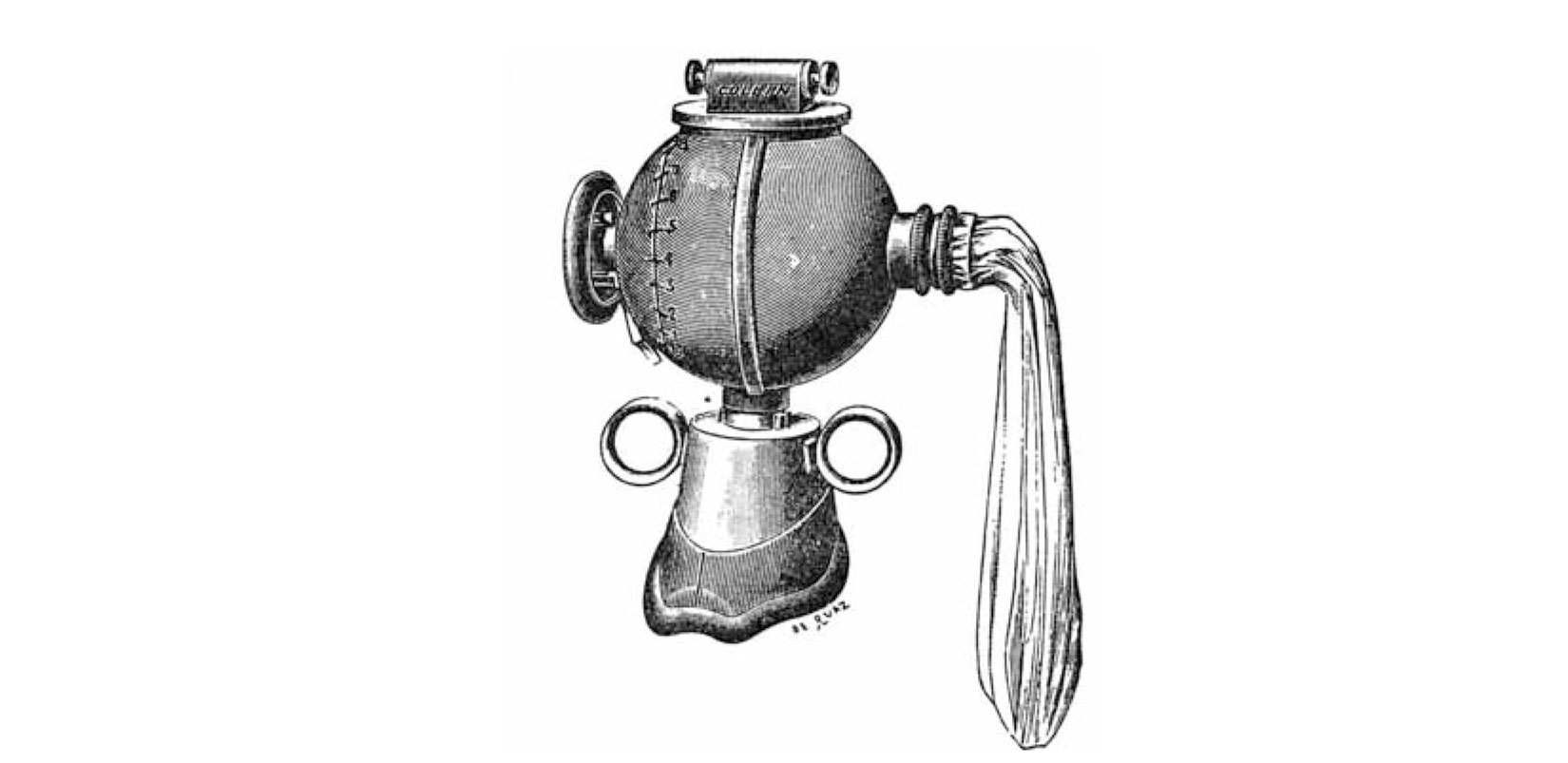
It took five years of experiments with M. Collin, the instrument maker, to achieve success. The final model (FIG.1) had a spherical body with a rebreathing bag on one side and a control knob moving a pointer up a scale on the other side. At the top was a cover which could be unscrewed for the introduction of ether, 150g lasting for one- and-a-half hours. Below was the mask fitted with two rings for the administrator’s thumbs, while the other fingers held up the chin: a very good fit was obtained in this way.
Internally (FIG. 2) a wide bore channelled from the control on the left to the bag on the right; an opening (A) in this channel allowed air to be drawn in on inspiration and two short ducts led upwards from the main channel and opened into the body of the inhaler, while another led down towards themask (B). The side channel (c)allowed rebreathing into the bag. The main channel was divided by a central septum and lined by a cylindrical drum, which was rotated by the control. When the pointer moved up the scale three changes took place : reduction in the size of opening A, opening of the ducts leading to the ether chamber and closing of the side channel c, so that increasingamounts of the rebreathed air went through the body of the inhaler.
Induction was begun with the ether turned off (FIG.2); in this position the patient inhaled air with partial rebreathing and no ether.
The pointer was moved up the scale at a rate which the patient would tolerateuntilthehalfwaystagewasreached(FIG. 3);herethemixture inhaled consisted of air and bag contents passing through the ether chamber and the side channel. This was the position generally used for maintenance, but a higher concentration was needed for induction and it was sometimes even necessary to move the pointer to the top of the scale (FIG. 4). A little air was still drawn in, but not enough to prevent the gradual appearance of cyanosis; the greater part of each breath came from the bag through the ether compartment and return- ed by the same route. This position was required only in resistant patients and then not for long. The area of the different openings had to be worked out with great care and was obtained by trial and error.
In practice this inhaler was found to work quite well. The original makers sold over 25,0002 and many imitations were sold by other firms. It is now largely obsolete if only because the respiration cannot be assisted.
Louis Ombredanne became Surgeon to the Paris Hospitals in 1902, Professeur AgrCgC in 1907 and was appointed to the Chair of Infantile Surgery and OrthopEdics (University of Paris) in 1925. He retired in 1941 and died in 1956.
Acknowledgements
My thanks are due to Miss M. Benstead for the diagrams and to Collin et Cie for the illustration.
References
‘OMBREDANNE, L. (1908). Gaz.Hap.,Paris,81,1095. * C O L L I N E T C I E (1959). Personal communication.